
General information
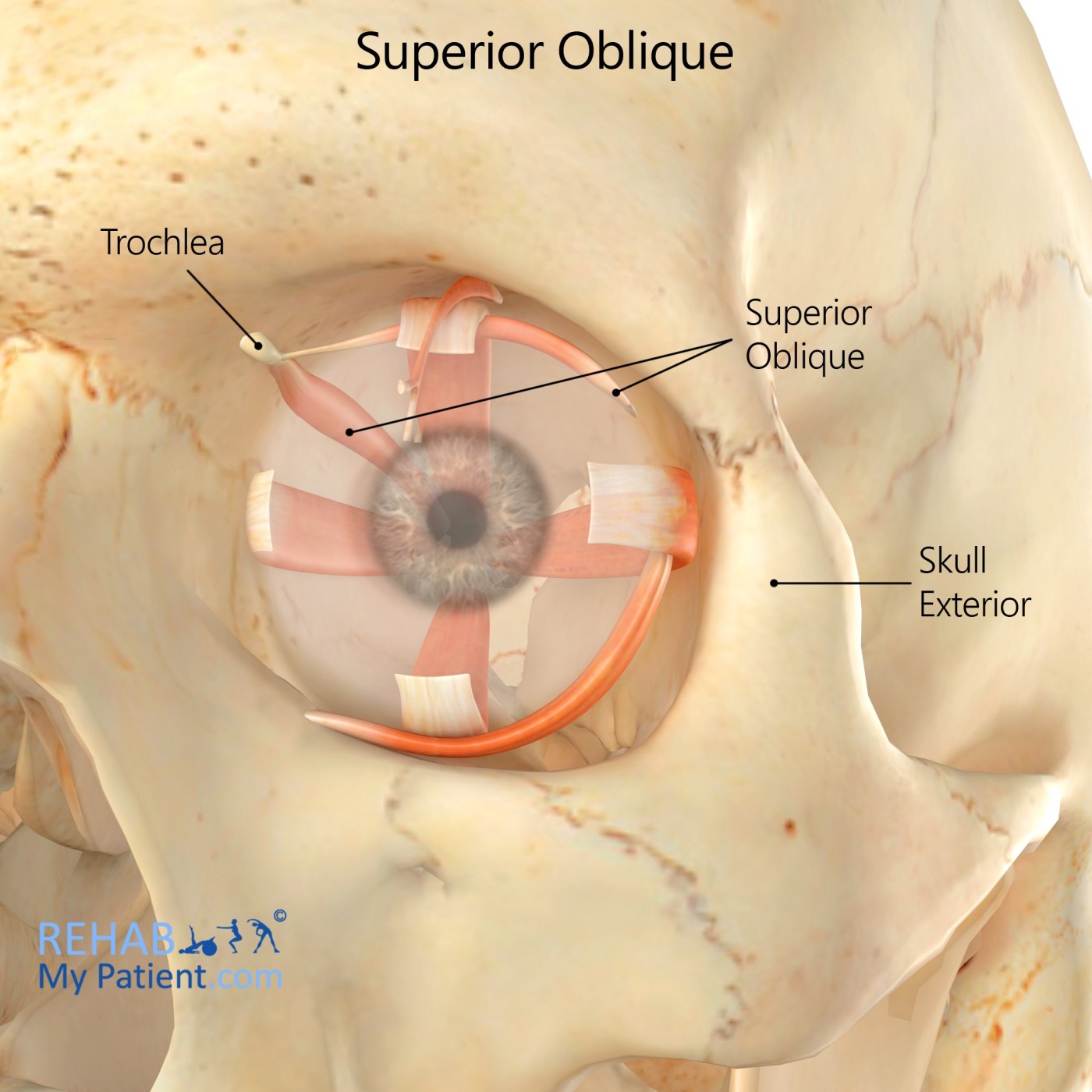
The superior oblique is a fusiform muscle that originates from the upper and medial side of the orbit. It controls depressing, abducting and internally rotating the eye. This muscle is the only extraocular muscle that is innervated from the trochlear nerve.
Literal meaning
Over and above.
Interesting information
The fourth cranial nerve is responsible for innervating the superior oblique, so any weakness in the nerve is referred to as superior oblique palsy. Weakness of the muscle causes horizontal, vertical and torsional misalignment for the eyes. This vertical misalignment is often one of the most notable features. Palsy is a complete weakness for the muscles while the paresis is a state of partial weakness. Most of the time, the condition is unilateral, but it can affect both eyes.
Superior oblique palsy can cause double vision due to the eyes being misaligned. The brain ends up perceiving images from multiple directions. The double vision could be vertical, diagonal and even torsional. Torsional tends to occur more often with those who have an acquired case of palsy. Head tilting tends to be common with this condition. It allows the individual to see better and align the eyes to provide relief to the patient. Children who go around tilting their head need to be evaluated for this condition to make sure the necessary treatment is provided.
Origin
Sphenoid bone superior and medial in relation to the optic canal.
Insertion
Passes through the trochlear loop and into the superolateral surface for the sclera in the posterior half.
Function
Abduction, depression and intorsion of the eye.
Nerve supply
Trochlear nerve.
Blood supply
Ophthalmic artery’s muscular branches from the internal carotid artery.
Relevant research
MRI studies for the superior oblique muscles have shown an increased incidence of muscle atrophy in congenital palsy patients. Reports indicate that long-standing palsy patients show atrophic muscles within the eye affected. The study’s purpose was to compare the incidence of muscle atrophy in congenital and acquired patients through the use of an MRI. Image planes were taken out of the 29 different congenital patients and the nine acquired unilateral patients. Muscle bellies were traced and the sizes were measured from the various image planes. The total volume of the muscle was compared to the normal eye. The reduction in volume for the congenital patients appeared to be a congenital abnormality instead of that of a secondary change, which was seen in a lot of the acquired palsy patients.
Sato M, Yagasaki T, Kora T, Awaya S. Comparison of muscle volume between congenital and acquired superior oblique palsies by magnetic resonance imaging. Jpn J Ophthalmol. 1998;42(6):466-470. doi:10.1016/s0021-5155(98)00044-6.
Superior oblique exercises
Figure eights
This exercise is great for strengthening the muscles in the eye to improve control and function. Sit or stand in a comfortable position. Trace an invisible figure 8 along the floor in front of you about eight to 10 feet in the distance without moving the head. Trace the lines in one direction and then switch to the other direction. Perform three to five sets of the exercise daily.
Sign Up
Sign up for your free trial now!
Get started with Rehab My Patient today and revolutionize your exercise prescription process for effective rehabilitation.
Start Your 14-Day Free Trial